Cavernoma
A cavernoma, or cavernous haemangioma, is a vascular malformation in the brain or spinal cord made up of a cluster of abnormal, closely packed, thin-walled capillaries. These "mulberry-like" structures contain slow-moving blood and can leak small amounts of fluid, leading to headaches, seizures, or neurological deficits.

Symptoms
- New-onset seizures (the most common presenting symptom).
- Recurrent headaches, which can range from mild to severe.
- Focal neurological deficits (weakness, numbness, vision changes) depending on the cavernoma's location.
- Balance and coordination problems, especially with brainstem cavernomas.
- Symptoms caused by minor recurrent bleeding into surrounding brain tissue.
 Clinical anatomical model showing affected spinal structures (no text).
Clinical anatomical model showing affected spinal structures (no text). Causes and risk factors
- Congenital: most cavernomas are present from birth.
- Genetic mutations: about 20% of cases are hereditary, often causing multiple cavernomas (familial cavernous malformation).
- Sporadic cases, which typically present as a single isolated cavernoma.
- History of prior brain radiation therapy in rare instances.
How diagnosis is made
- Brain MRI (specifically gradient echo or susceptibility-weighted imaging) is the definitive diagnostic method showing the "popcorn" appearance.
- CT scan to detect acute haemorrhage or calcification.
- Catheter angiograms are typically negative (cavernomas are "low-flow" lesions).
 Typical diagnostic grey-scale imaging scan (MRI/CT).
Typical diagnostic grey-scale imaging scan (MRI/CT). Non-surgical treatment options
- Observation with serial MRI scans for asymptomatic or stable cavernomas.
- Anti-seizure medications to manage and prevent seizures.
- Avoidance of blood-thinning medications when clinically safe.
- Lifestyle modifications and regular clinical follow-up.
When surgery may be considered
Surgical resection (microsurgical excision) is considered for cavernomas that cause recurrent, drug-resistant seizures, progressive neurological deficits, or have caused multiple documented symptomatic haemorrhages, provided they are in a surgically accessible location.
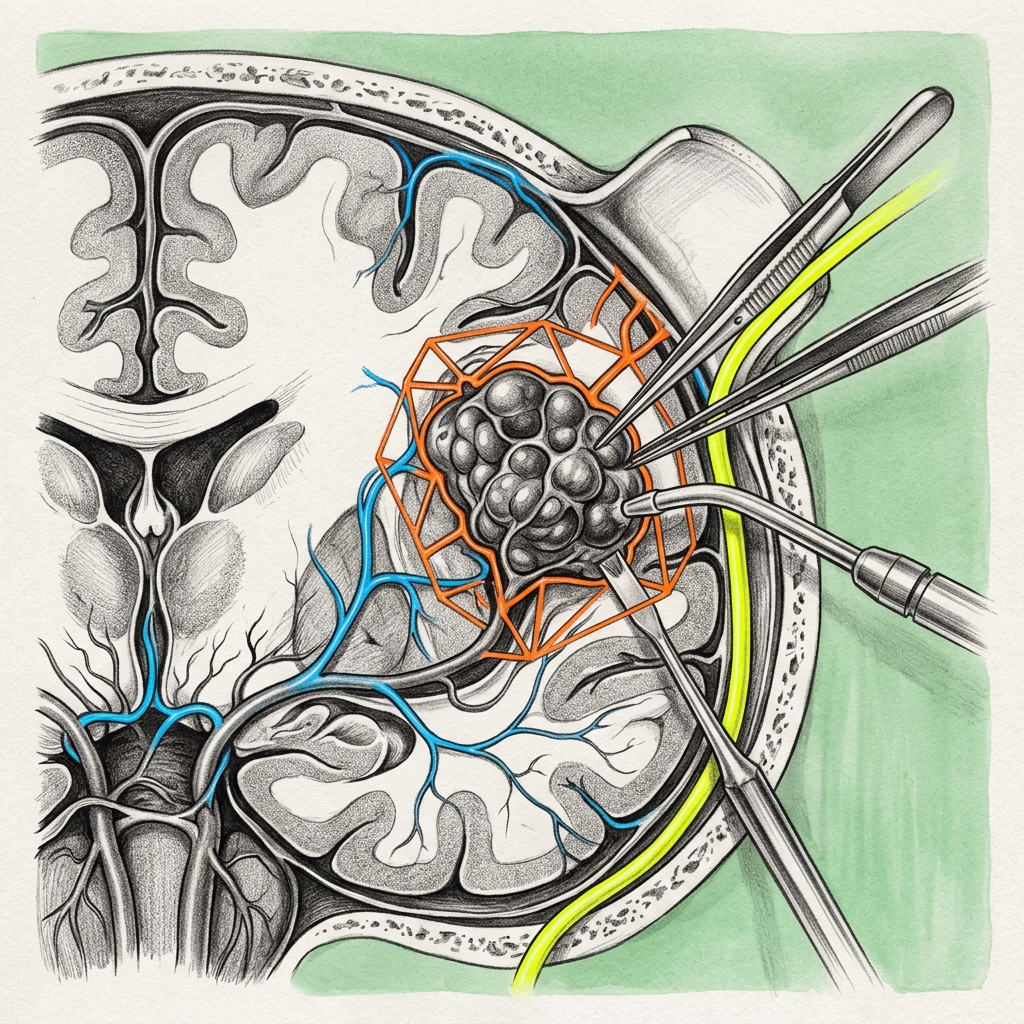 Advanced surgical technology and precision instrumentation.
Advanced surgical technology and precision instrumentation. Expected outcomes
Complete surgical removal of accessible cavernomas is highly successful, curative, and eliminates the future risk of bleeding and seizures. Brainstem or deep-seated cavernomas carry higher surgical risks and require careful multidisciplinary planning.
 Rehabilitation pathways and safe movement restoration.
Rehabilitation pathways and safe movement restoration. Frequently asked questions
Can a cavernoma run in families?
Yes. In about 20% of cases, cavernomas are inherited in an autosomal dominant pattern. Familial cavernomas are often characterised by multiple lesions throughout the brain and require genetic counselling.