Pituitary Tumour
A pituitary tumour (pituitary adenoma) is a usually benign growth arising from the pituitary gland at the base of the brain. Pituitary tumours can cause hormonal imbalances and, when large enough, compress the optic nerves leading to visual loss. They are among the most common intracranial tumours.

Symptoms
- Visual field loss, classically bitemporal hemianopia (loss of peripheral vision on both sides).
- Headaches, often dull and persistent.
- Hormonal excess symptoms depending on tumour type: irregular periods, infertility, milk production (prolactinoma), acromegaly (growth hormone), Cushing syndrome (ACTH).
- Hormonal deficiency symptoms: fatigue, weight changes, loss of libido, cold intolerance.
- Double vision if the tumour extends into the cavernous sinus.
- Sudden severe headache with rapid visual loss if pituitary apoplexy (haemorrhage into the tumour) occurs.
 Clinical anatomical model showing affected spinal structures (no text).
Clinical anatomical model showing affected spinal structures (no text). Causes and risk factors
- The exact cause of most pituitary adenomas is unknown.
- Genetic syndromes: Multiple Endocrine Neoplasia type 1 (MEN1), Carney complex, familial isolated pituitary adenoma (FIPA).
- Most pituitary adenomas are sporadic and not inherited.
- Pituitary tumours are common, found incidentally in up to 10% of MRI scans.
How diagnosis is made
- MRI of the pituitary with dedicated thin-cut sequences and contrast enhancement.
- Comprehensive blood tests for pituitary hormones: prolactin, growth hormone, IGF-1, cortisol, ACTH, thyroid function, gonadotropins.
- Formal visual field testing (perimetry) to assess optic nerve compression.
- CT scan in emergency presentations, particularly for pituitary apoplexy.
 Typical diagnostic grey-scale imaging scan (MRI/CT).
Typical diagnostic grey-scale imaging scan (MRI/CT). Non-surgical treatment options
- Prolactinomas: dopamine agonist medication (cabergoline or bromocriptine) is the first-line treatment and shrinks the tumour in most cases.
- Observation with serial MRI and hormone monitoring for small, non-functioning, asymptomatic tumours (incidentalomas).
- Hormone replacement therapy for pituitary hormone deficiencies.
- Radiotherapy (stereotactic radiosurgery) for residual or recurrent tumour after surgery.
When surgery may be considered
Transsphenoidal surgery (through the nose) is recommended for pituitary tumours causing visual compromise, hormonal excess not controlled by medication (particularly growth hormone and ACTH-producing tumours), or significant tumour growth on serial imaging.
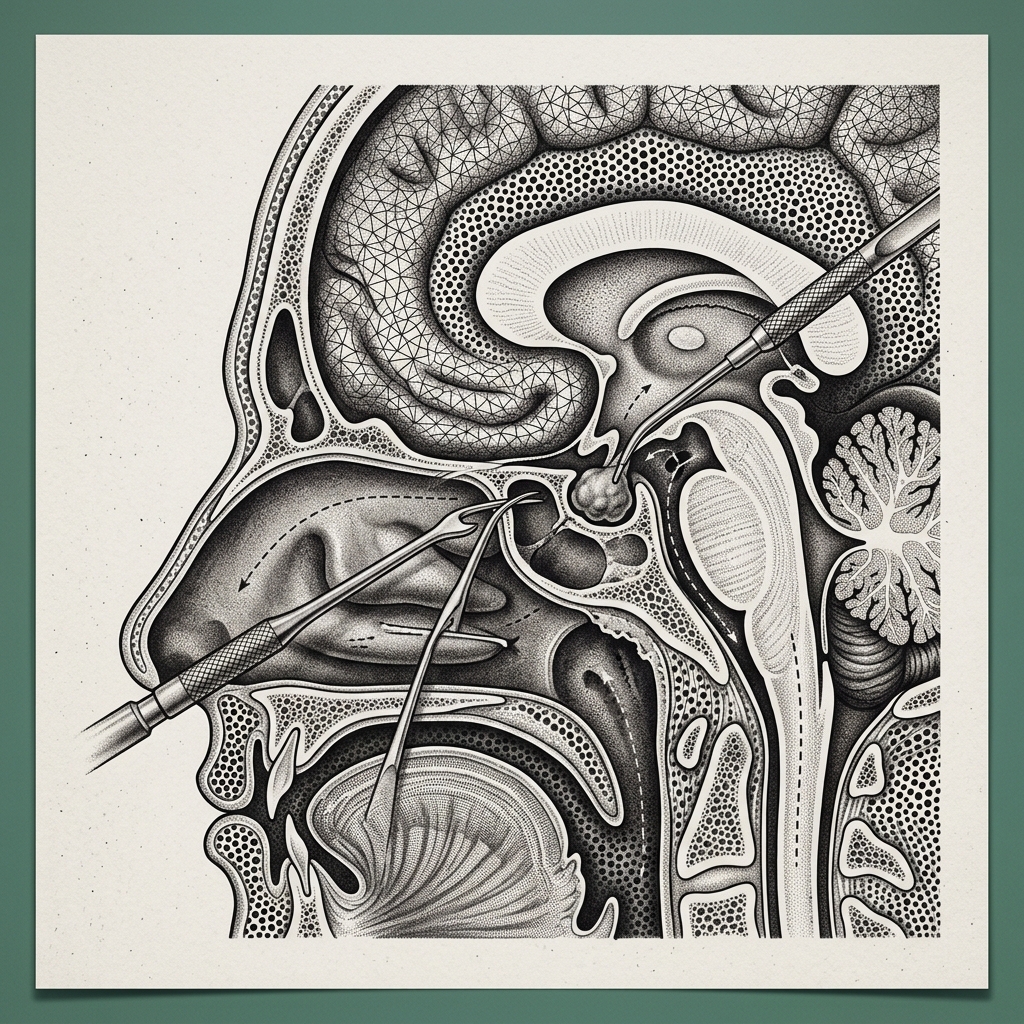 Advanced surgical technology and precision instrumentation.
Advanced surgical technology and precision instrumentation. Expected outcomes
Transsphenoidal pituitary surgery is highly effective, with tumour removal rates exceeding 80% for most adenomas. Visual improvement occurs in the majority of patients with pre-operative visual loss. Hormonal cure rates vary by tumour type. The procedure has a low complication rate in experienced hands.
 Rehabilitation pathways and safe movement restoration.
Rehabilitation pathways and safe movement restoration. Frequently asked questions
Are pituitary tumours cancerous?
The vast majority (over 99%) of pituitary tumours are benign adenomas. Pituitary carcinoma is exceedingly rare. However, even benign pituitary tumours can cause significant problems through hormone excess or compression of nearby structures like the optic nerves.
Will I need hormone replacement after pituitary surgery?
Some patients require temporary or permanent hormone replacement after pituitary surgery, particularly if the tumour has damaged normal pituitary tissue. Your endocrinologist will monitor hormone levels closely after surgery and prescribe replacement as needed.