Peripheral Nerve Tumours
Peripheral nerve tumours are growths that develop within or along the nerves outside the brain and spinal cord. The most common types are schwannomas and neurofibromas, which are usually benign. They can cause pain, weakness, or a palpable lump along the course of a nerve. Surgical excision is typically curative.

Symptoms
- A palpable, firm lump or mass along the course of a peripheral nerve.
- Pain or tenderness at the tumour site, which may radiate along the nerve distribution.
- Tingling, numbness, or electric-shock sensations (Tinel sign) when the mass is tapped.
- Progressive weakness in the muscles supplied by the affected nerve.
- Slow growth over months to years is typical for benign tumours.
- Rapid growth, severe pain, or new neurological deficit may suggest malignancy.
 Clinical anatomical model showing affected spinal structures (no text).
Clinical anatomical model showing affected spinal structures (no text). Causes and risk factors
- Schwannomas arise from Schwann cells (the insulating sheath around nerves) and are almost always benign.
- Neurofibromas arise from a mix of nerve cell types and are usually benign but can undergo malignant transformation.
- Neurofibromatosis type 1 (NF1) and type 2 (NF2) are genetic conditions associated with multiple nerve tumours.
- Schwannomatosis is a rare genetic condition causing multiple schwannomas.
- Malignant peripheral nerve sheath tumours (MPNSTs) are rare but more common in patients with NF1.
- Most sporadic solitary schwannomas occur without a known genetic cause.
How diagnosis is made
- Clinical examination including assessment of nerve function and Tinel sign at the tumour site.
- MRI with contrast to characterise the tumour, define its relationship to the nerve, and plan surgery.
- Ultrasound for superficial nerve tumours and to guide biopsy if needed.
- Nerve conduction studies and EMG to assess the functional impact on the nerve.
- Biopsy is sometimes needed but is usually deferred until surgical excision to avoid nerve damage.
 Typical diagnostic grey-scale imaging scan (MRI/CT).
Typical diagnostic grey-scale imaging scan (MRI/CT). Non-surgical treatment options
- Observation with serial imaging for small, asymptomatic tumours.
- Pain management with neuropathic pain medications (gabapentin, pregabalin).
- Monitoring for changes in size, symptoms, or nerve function.
When surgery may be considered
Surgical excision is recommended for symptomatic peripheral nerve tumours (pain, weakness, numbness), growing tumours, or when malignancy cannot be excluded. Microsurgical techniques allow most benign tumours to be removed while preserving nerve function.
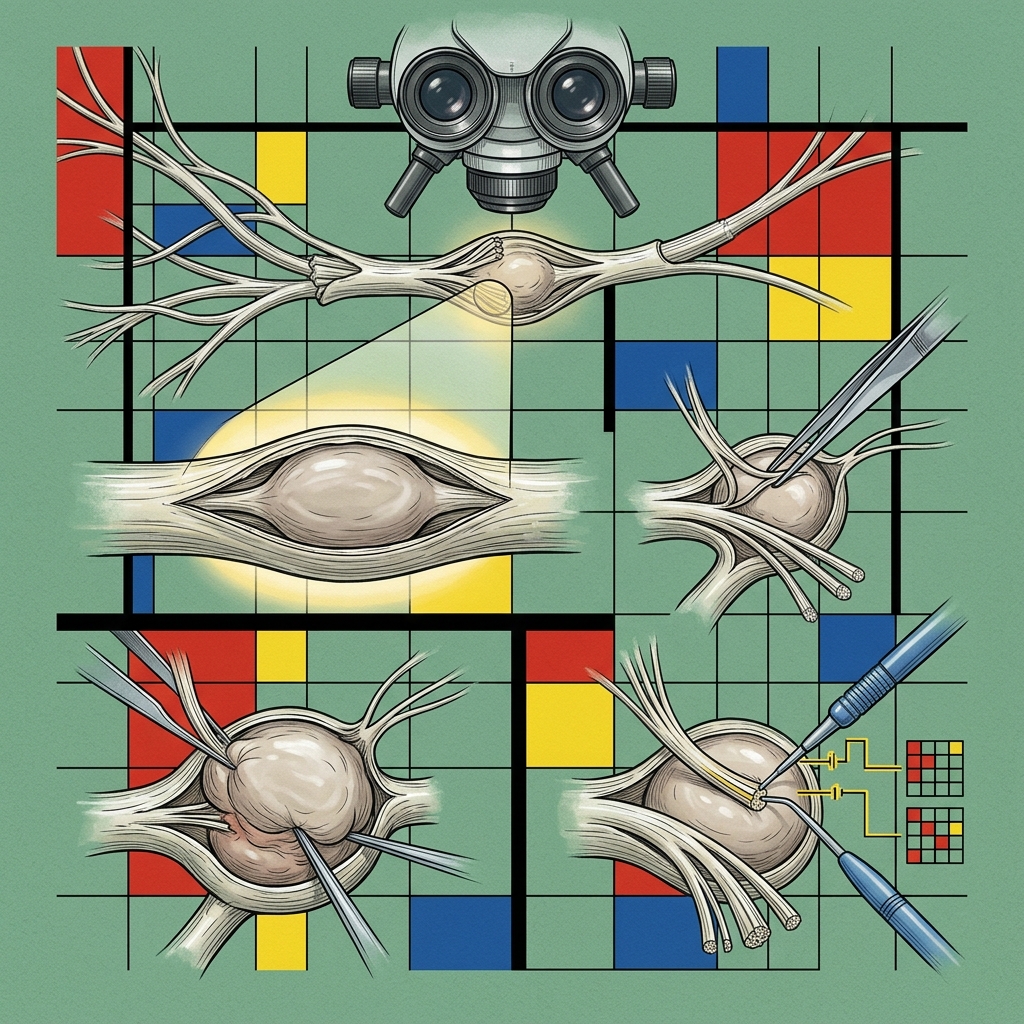 Advanced surgical technology and precision instrumentation.
Advanced surgical technology and precision instrumentation. Expected outcomes
Microsurgical excision of schwannomas is curative in the vast majority of cases with excellent preservation of nerve function. Neurofibromas are more challenging because they are interwoven with nerve fibres, but experienced microsurgical technique minimises neurological deficit. Recurrence of benign tumours is uncommon.
 Rehabilitation pathways and safe movement restoration.
Rehabilitation pathways and safe movement restoration. Frequently asked questions
Can peripheral nerve tumours become cancerous?
Most peripheral nerve tumours (schwannomas and solitary neurofibromas) are benign and do not become cancerous. However, patients with neurofibromatosis type 1 (NF1) have an increased lifetime risk of malignant peripheral nerve sheath tumour (MPNST). Rapid growth or new severe pain should prompt urgent reassessment.
Will I lose nerve function after tumour removal?
Microsurgical techniques allow most schwannomas to be separated from the nerve with preservation of function. Some temporary numbness or weakness may occur after surgery but usually recovers. The risk of permanent deficit depends on tumour type, size, and location.