Spinal Stenosis
Spinal stenosis is a narrowing of the spinal canal that places pressure on the spinal cord and nerves. It most commonly affects the lumbar (lower back) and cervical (neck) regions, leading to pain, numbness, or weakness in the legs or arms.

Symptoms
- Leg pain, heaviness, or cramping that worsens with walking or standing (neurogenic claudication).
- Improvement of symptoms when sitting, leaning forward, or bending at the waist.
- Numbness or tingling in the legs, feet, arms, or hands depending on the level affected.
- Gradual loss of balance and unsteadiness when walking.
- In cervical stenosis: hand clumsiness, difficulty with fine motor tasks, and gait disturbance.
- In severe cases, bladder or bowel dysfunction.
 Clinical anatomical model showing affected spinal structures (no text).
Clinical anatomical model showing affected spinal structures (no text). Causes and risk factors
- Age-related degenerative changes including disc bulging, ligament thickening, and facet joint enlargement.
- Bone spurs (osteophytes) growing into the spinal canal.
- Thickening of the ligamentum flavum reducing available space for the spinal cord and nerves.
- Degenerative spondylolisthesis where one vertebra slips forward on another.
- Congenital spinal canal narrowing (less common).
- Previous spinal surgery or trauma leading to scarring and narrowing.
How diagnosis is made
- Clinical examination assessing walking pattern, balance, reflexes, and sensation.
- MRI scan to visualise the degree and location of canal narrowing and nerve compression.
- CT scan with or without myelography for detailed assessment of bony anatomy.
- X-rays including flexion-extension views to assess spinal stability.
- Nerve conduction studies when the clinical picture is complex.
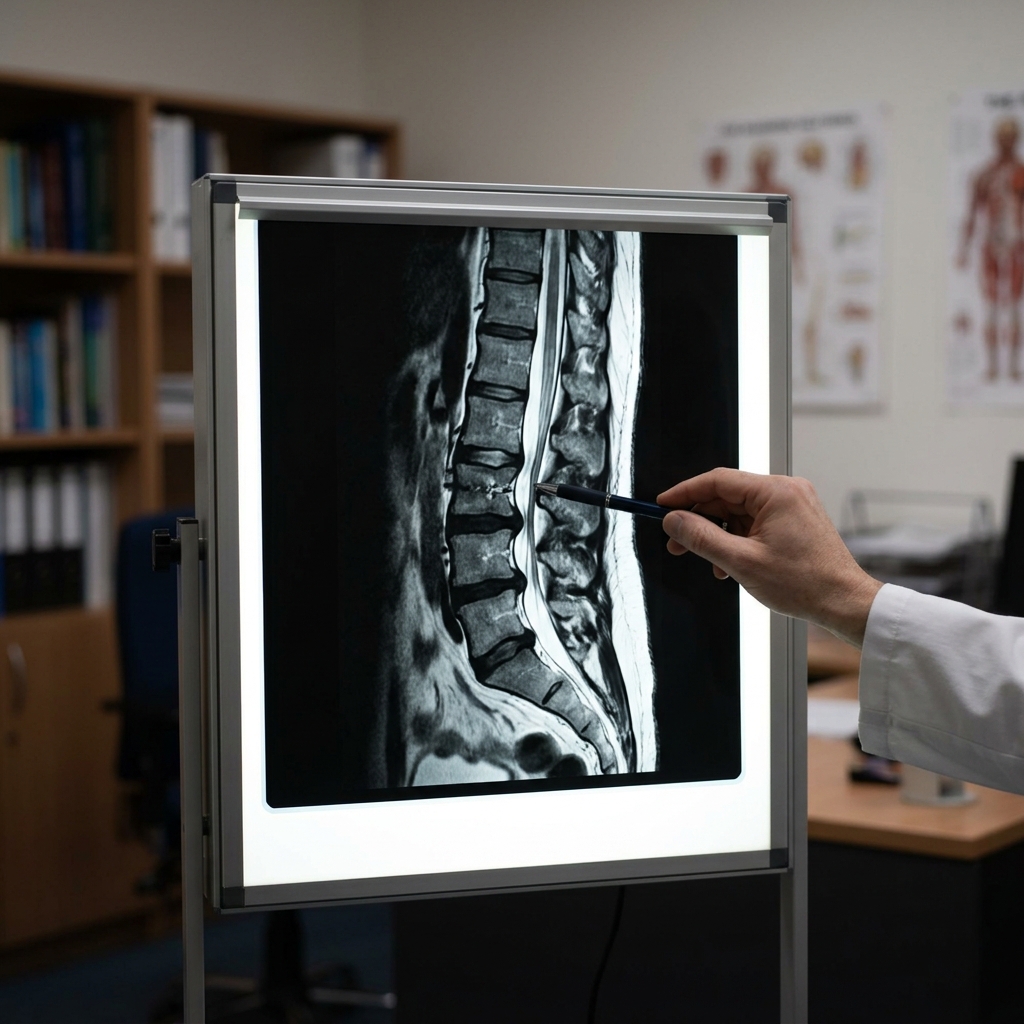 Typical diagnostic grey-scale imaging scan (MRI/CT).
Typical diagnostic grey-scale imaging scan (MRI/CT). Non-surgical treatment options
- Physiotherapy focusing on core strengthening, flexibility, and postural training.
- Anti-inflammatory and neuropathic pain medications.
- Epidural steroid injections to reduce nerve inflammation and provide temporary relief.
- Activity modification, including using a walking frame or trolley for support.
- Weight management to reduce spinal load.
When surgery may be considered
Surgery is considered when conservative measures fail to adequately control symptoms, when walking tolerance is significantly reduced, or when there is evidence of progressive neurological decline. Decompressive surgery (laminectomy or laminoplasty) relieves pressure on the nerves and can significantly improve walking ability and quality of life.
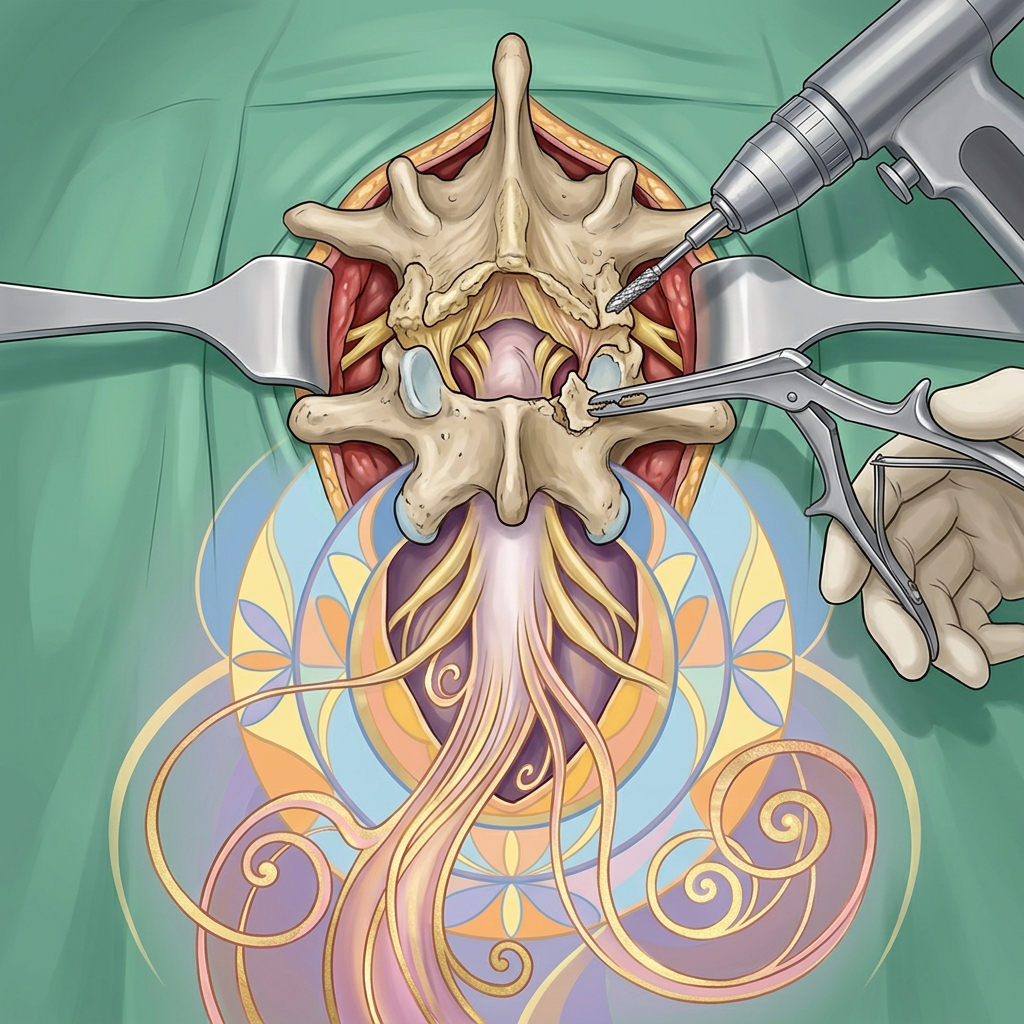 Advanced surgical technology and precision instrumentation.
Advanced surgical technology and precision instrumentation. Expected outcomes
Decompressive surgery for lumbar stenosis reliably improves walking tolerance and reduces leg pain in approximately 80 to 85% of patients. Cervical stenosis surgery can halt progression and improve hand function and balance. Long-term outcomes are generally favourable.
 Rehabilitation pathways and safe movement restoration.
Rehabilitation pathways and safe movement restoration. Frequently asked questions
Does spinal stenosis always require surgery?
No. Many patients manage their symptoms effectively with physiotherapy, medication, and lifestyle adjustments. Surgery is reserved for cases where conservative treatment does not provide adequate relief or neurological function is declining.
Can spinal stenosis get worse over time?
Spinal stenosis is typically a slowly progressive condition. Some patients remain stable for years, while others experience gradual worsening. Regular clinical review helps monitor progression.
What is the recovery time after spinal stenosis surgery?
Most patients are walking within hours of surgery and are discharged within 1 to 3 days. Significant improvement in walking and leg symptoms is usually noticed within the first few weeks, with full recovery over 3 to 6 months.