Peripheral Nerve Injury
Peripheral nerve injuries result from trauma, compression, or laceration to the nerves outside the brain and spinal cord. They can cause numbness, weakness, or complete loss of function in the affected limb. Timely diagnosis and appropriate surgical repair or reconstruction are critical for optimal recovery.

Symptoms
- Sudden numbness or loss of sensation in the distribution of the injured nerve.
- Weakness or complete paralysis of muscles supplied by the nerve.
- Burning, shooting, or electric-shock pain (neuropathic pain).
- Loss of reflexes in the affected area.
- Muscle wasting (atrophy) over time if the nerve does not recover.
- Trophic changes in the skin: dryness, hair loss, and nail changes in the denervated area.
 Clinical anatomical model showing affected spinal structures (no text).
Clinical anatomical model showing affected spinal structures (no text). Causes and risk factors
- Lacerations from sharp trauma (glass, knife, machinery).
- Fractures and dislocations causing nerve stretch or compression.
- Gunshot wounds and blast injuries.
- Traction injuries (brachial plexus injuries from motorcycle accidents or birth trauma).
- Iatrogenic injury (during surgery).
- Compression neuropathy from prolonged pressure (crutch palsy, tourniquet injury, Saturday night palsy).
How diagnosis is made
- Clinical examination to map the pattern of sensory loss and motor weakness to identify the injured nerve.
- Nerve conduction studies and electromyography (EMG), typically performed 3 to 4 weeks after injury to assess the degree of nerve damage.
- Ultrasound for superficial nerve injuries to visualise nerve continuity.
- MRI neurography for deeper nerve injuries or brachial plexus assessment.
- Surgical exploration when the nerve injury mechanism suggests complete transection.
 Typical diagnostic grey-scale imaging scan (MRI/CT).
Typical diagnostic grey-scale imaging scan (MRI/CT). Non-surgical treatment options
- Observation and serial clinical/electrophysiological assessment for closed injuries with a potential for spontaneous recovery (neurapraxia, some axonotmesis).
- Splinting to prevent joint contractures while awaiting nerve recovery.
- Physiotherapy to maintain joint range of motion and prevent muscle wasting.
- Neuropathic pain management with gabapentin, pregabalin, or amitriptyline.
- Occupational therapy for adaptive strategies and aids.
When surgery may be considered
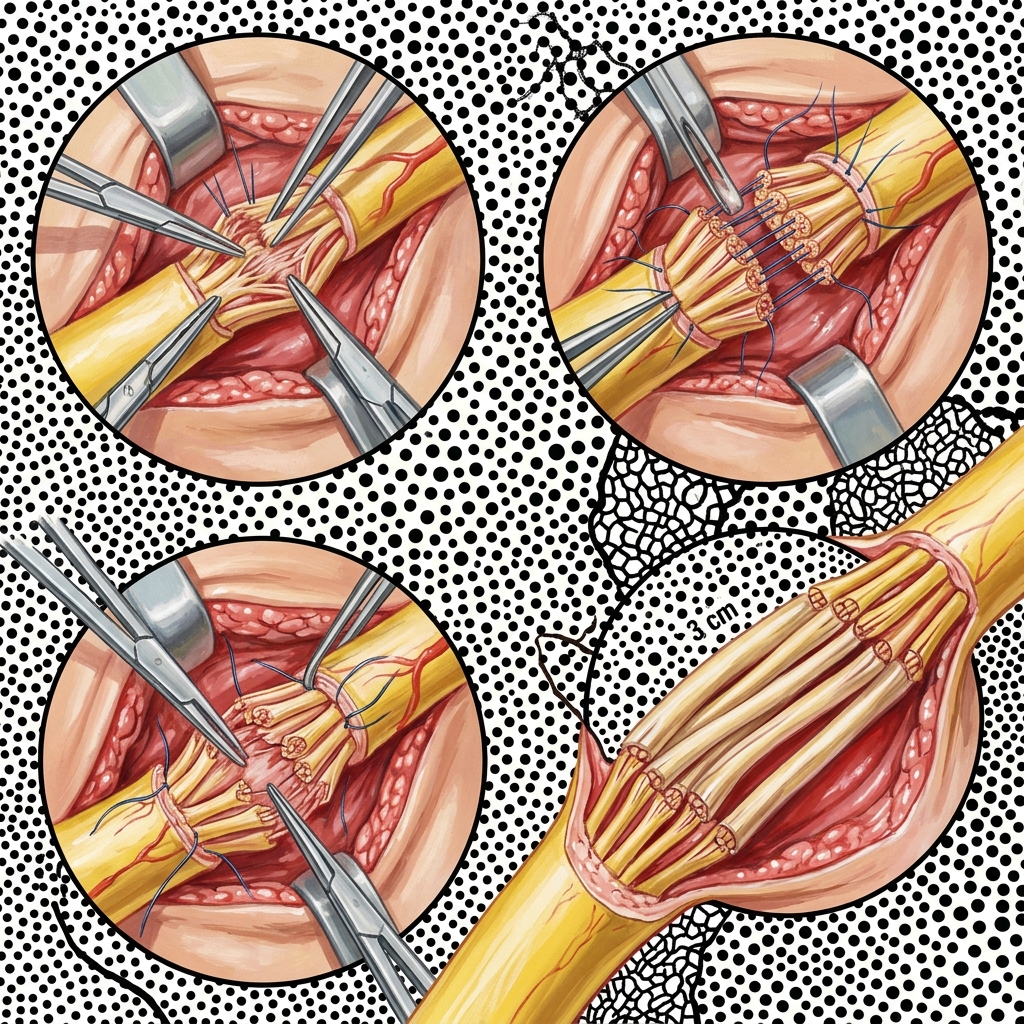
Surgical repair is indicated for sharp nerve transections (primary repair), failed nerve recovery after closed injuries (nerve grafting or transfer), and nerve compression not responding to conservative measures. The timing of surgery is critical: primary repair within 72 hours for sharp lacerations, and exploration by 3 to 6 months if a closed nerve injury shows no clinical or electrophysiological recovery.
 Advanced surgical technology and precision instrumentation.
Advanced surgical technology and precision instrumentation. Expected outcomes
Outcomes depend on the type and severity of nerve injury, the nerve involved, the patient's age, and the timing of repair. Sharp nerve repairs performed early have the best prognosis. Nerve grafts and transfers can restore meaningful function even in severe injuries. Recovery is slow, as nerves regenerate at approximately 1 mm per day.
 Rehabilitation pathways and safe movement restoration.
Rehabilitation pathways and safe movement restoration. Frequently asked questions
How long does it take for a nerve to grow back after repair?
Peripheral nerves regenerate at approximately 1 mm per day (about 2.5 cm per month). The time to recovery depends on the distance from the repair site to the target muscle or skin. For example, a nerve repaired at the wrist may take 3 to 6 months to reach the hand, while a repair at the shoulder may take 12 to 18 months to reach the forearm muscles.
What happens if a nerve injury is not repaired?
An unrepaired nerve transection will not recover spontaneously. Over time, the muscles it supplies will atrophy irreversibly (typically after 18 to 24 months), and the chance of successful surgical recovery diminishes significantly. This is why timely diagnosis and referral are critical.