Herniated Disc
A herniated disc occurs when the soft, gel-like centre of a spinal disc pushes through a tear in the tougher outer layer. This can press on nearby nerves, causing pain, numbness, or weakness in the arm or leg.

Symptoms
- Sharp or burning pain in the neck, back, arm, or leg depending on the location of the herniation.
- Numbness or tingling radiating into the arm (cervical) or leg (lumbar).
- Muscle weakness in the affected limb, making it difficult to lift objects or walk steadily.
- Pain that worsens with sitting, coughing, sneezing, or bending forward.
- In severe cases, difficulty with bladder or bowel control (seek urgent care immediately).
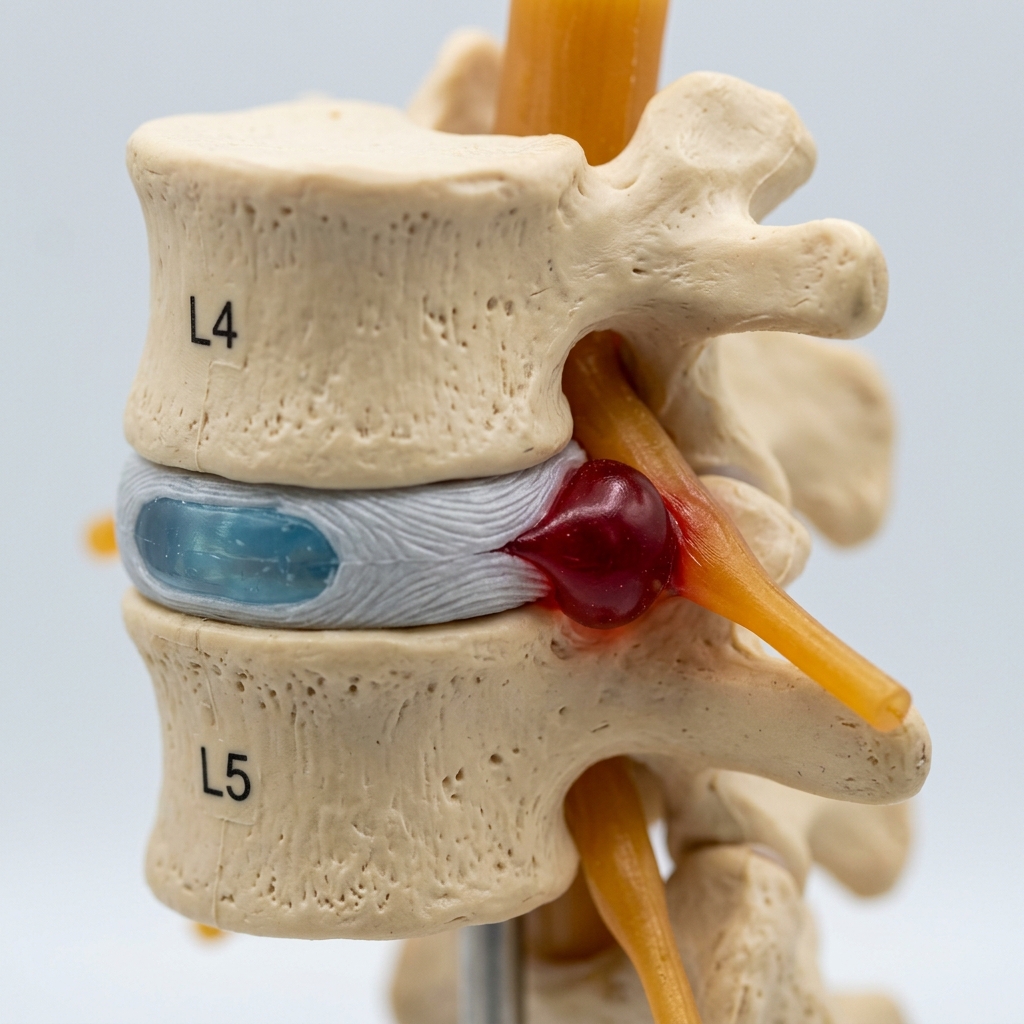 Clinical anatomical model showing affected spinal structures (no text).
Clinical anatomical model showing affected spinal structures (no text). Causes and risk factors
- Age-related disc degeneration and reduced water content in the disc.
- Heavy lifting or sudden twisting movements placing excess stress on the spine.
- Repetitive bending, lifting, or vibration through occupational or sporting activities.
- Excess body weight increasing the load on lumbar discs.
- Genetic predisposition to disc degeneration.
- Smoking, which impairs disc nutrition and accelerates degeneration.
How diagnosis is made
- Clinical assessment of symptoms, reflexes, muscle strength, and sensation patterns.
- MRI scan to visualise the disc herniation and identify which nerve is compressed.
- CT scan when MRI is not available or additional bony detail is required.
- Nerve conduction studies if the clinical picture is unclear or multiple levels are involved.
 Typical diagnostic grey-scale imaging scan (MRI/CT).
Typical diagnostic grey-scale imaging scan (MRI/CT). Non-surgical treatment options
- Activity modification and avoidance of aggravating movements during the acute phase.
- Physiotherapy focusing on core stabilisation, gentle stretching, and postural correction.
- Oral pain relief including anti-inflammatory medications and neuropathic pain agents.
- Epidural corticosteroid injections to reduce inflammation around the compressed nerve.
- Time: many herniated discs improve within 6 to 12 weeks with conservative management.
When surgery may be considered
Surgery may be considered when significant pain, numbness, or weakness persists despite 6 to 12 weeks of conservative treatment, or earlier if there is progressive neurological deficit. Microdiscectomy or endoscopic discectomy can relieve nerve compression with a high success rate and rapid recovery.
 Advanced surgical technology and precision instrumentation.
Advanced surgical technology and precision instrumentation. Expected outcomes
Most patients experience significant pain relief after surgery, with microdiscectomy success rates typically exceeding 90% for leg pain. Return to normal activities usually occurs within 4 to 6 weeks. Recurrence risk is approximately 5 to 10% over the long term.
 Rehabilitation pathways and safe movement restoration.
Rehabilitation pathways and safe movement restoration. Frequently asked questions
Can a herniated disc heal without surgery?
Yes. The majority of herniated discs improve with conservative treatment including physiotherapy, medication, and activity modification. Surgery is only considered when symptoms persist or worsen despite adequate non-surgical care.
How long does recovery take after disc surgery?
Most patients are mobile on the day of surgery and return home within 24 hours. Return to desk work typically occurs within 2 to 4 weeks, and full activity within 6 to 12 weeks depending on the type of work.
What is the difference between a bulging disc and a herniated disc?
A bulging disc extends outward evenly beyond its normal boundary but the outer layer remains intact. A herniated disc involves a tear in the outer layer allowing the inner material to protrude, which is more likely to compress a nerve.