Awake Craniotomy
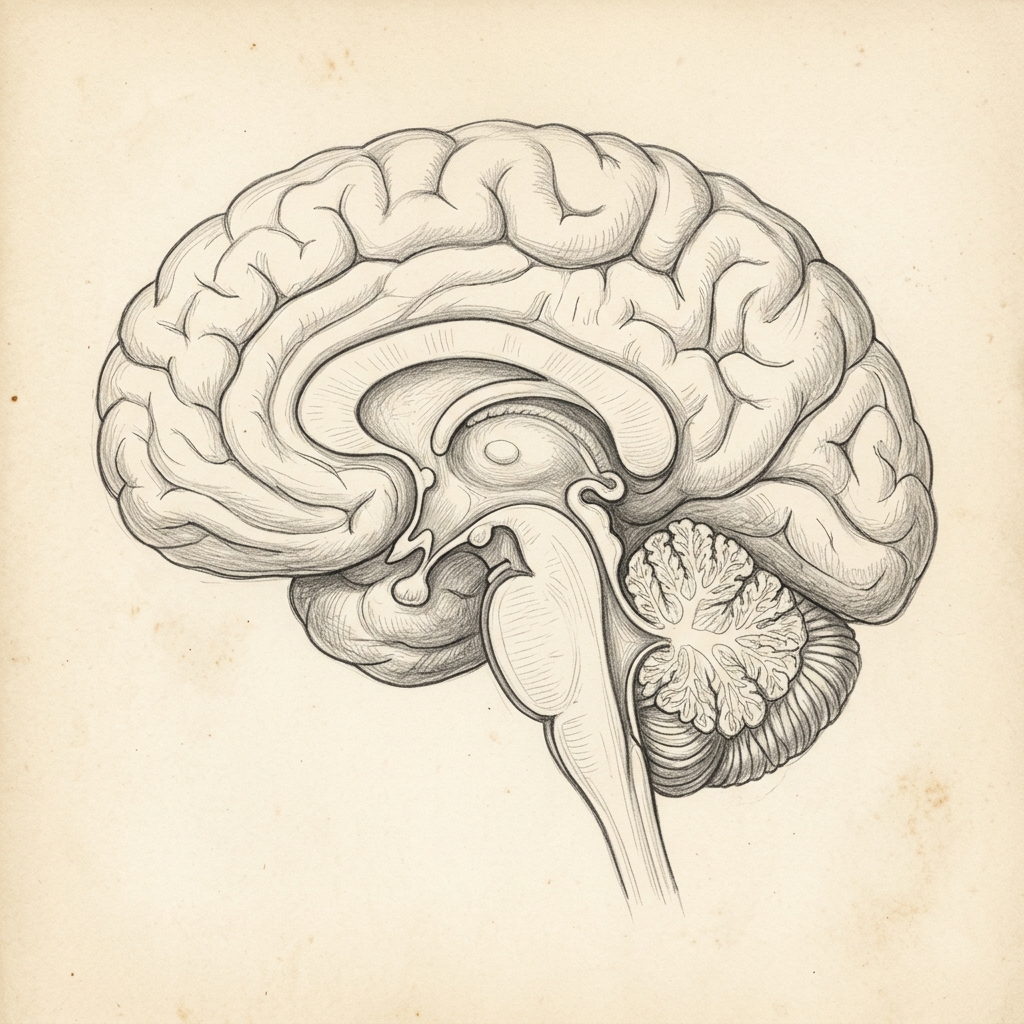
An awake craniotomy is a highly specialized neurosurgical procedure performed to remove brain tumours located within or immediately adjacent to critical functional areas of the brain, such as those controlling speech, language, movement, or sensation. By keeping the patient awake and conversing for a portion of the surgery, the neurosurgeon can map and monitor these eloquent pathways in real time, maximizing tumour resection while absolutely minimizing the risk of permanent neurological damage.
When this procedure may be recommended
- Gliomas, astrocytomas, or cavernomas located in eloquent brain areas (speech centres, motor strip).
- Intractable epilepsy requiring resection of seizure focus near critical brain structures.
- Surgical lesions requiring precise functional mapping to preserve speech, motor control, or sensory processing.
Who may be a candidate
Candidates must have a lesion located in a critical eloquent zone of the brain. They must be psychologically resilient, highly cooperative, and able to remain calm and follow instructions during intraoperative functional testing. Factors like severe anxiety, cognitive deficits, or certain airway conditions may preclude awake surgery.
 Advanced medical implant technology (no text).
Advanced medical implant technology (no text). Alternatives to surgery
- Standard craniotomy under general anaesthesia with asleep neuromonitoring (less precise for speech/language mapping).
- Stereotactic biopsy followed by radiotherapy or chemotherapy (if surgical resection is deemed too high-risk).
- Conservative observation with serial MRI scan monitoring.
What to expect
- Preparation & Sedation: The patient is initially sedated and local anaesthetic blocks are applied to the scalp to ensure complete pain relief. A customized head frame stabilizes the head.
- Access (Asleep Phase): The scalp incision is made, and a temporary window in the skull (craniotomy) is opened while the patient is comfortably sedated.
- Waking the Patient: The sedation is turned off, and the patient is gently awakened. They feel no pain in the brain tissue itself, as the brain does not have pain receptors.
- Brain Mapping: The neurosurgeon uses a tiny electrical probe to gently stimulate brain tissue while a neuropsychologist tests the patient’s speech, language, movement, or vision.
- Tumour Resection: The surgeon removes the tumour along safe boundaries, continuously interacting with the patient to verify that speech and motor pathways remain perfectly functional.
- Closing (Asleep Phase): The patient may be lightly re-sedated while the skull bone window is secured back in place and the scalp is closed.
Technology and imaging
Uses advanced cortical and subcortical stimulation mapping, high-resolution operating microscopes, image-guided neuronavigation, and real-time intraoperative neuropsychological testing.
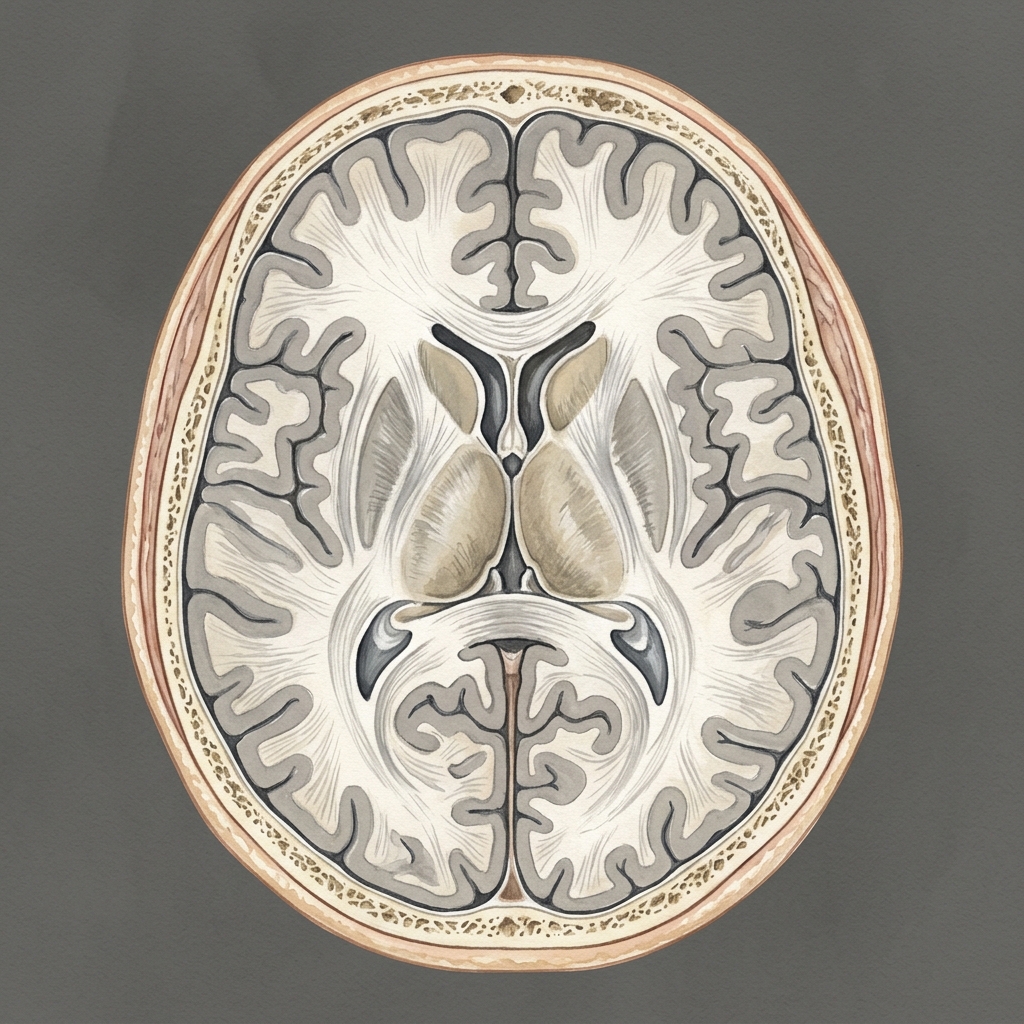 High-precision diagnostic imaging visualization.
High-precision diagnostic imaging visualization.  Clinical Zeiss/Leica operating microscope setup.
Clinical Zeiss/Leica operating microscope setup. Hospital stay
Usually 3 to 5 nights in hospital, including the first night in the Intensive Care Unit (ICU) or High Dependency Unit (HDU).
Recovery milestones
- ICU Stay (Day 1): Overnight monitoring to track neurological function, manage blood pressure, and control headaches.
- Ward Mobilisation (Days 2-4): Gentle walking, speech therapy reviews, and progressive recovery.
- Weeks 1-4: Home rest. Avoid strenuous activity, heavy lifting, or driving. Mild fatigue and scalp numbness are common.
- Weeks 6+: Follow-up MRI scan and clinical consultation to determine the necessity of any further oncological treatments.
 Post-operative mobilization and recovery milestones.
Post-operative mobilization and recovery milestones. Risks and complications
- Transient neurological deficit (e.g., temporary speech difficulties or arm/leg weakness, resolving in weeks).
- Intraoperative seizure (5% risk, managed immediately with cold irrigation on the brain).
- Brain swelling or bleeding (hematoma).
- Infection, cerebrospinal fluid leak, or wound healing delay.
Frequently asked questions
Will I feel pain while awake during surgery?
No. The scalp and skull are thoroughly numbed with long-acting local anaesthetics before surgery, and the brain itself has no pain receptors, meaning you will not feel any pain when the tumour is being mapped or removed.
What if I panic during the awake phase?
The surgical team, including a specialized anaesthetist and neuropsychologist, is by your side the entire time to support you. Sedation can be adjusted immediately, and if necessary, you can be safely put to sleep at any stage of the procedure.