Radiculopathy
Radiculopathy refers to compression or irritation of a spinal nerve root as it exits the spinal column. This produces pain, numbness, tingling, or weakness that radiates along the path of the affected nerve into the arm (cervical radiculopathy) or leg (lumbar radiculopathy).

Symptoms
- Radiating pain from the neck into the shoulder, arm, and hand (cervical) or from the lower back into the buttock and leg (lumbar).
- Numbness or tingling following a specific nerve distribution pattern (dermatome).
- Muscle weakness in the arm or leg supplied by the affected nerve root.
- Reduced reflexes at the elbow, wrist, knee, or ankle depending on the level.
- Pain often worsened by certain head positions (cervical) or sitting and bending (lumbar).
 Clinical anatomical model showing affected spinal structures (no text).
Clinical anatomical model showing affected spinal structures (no text). Causes and risk factors
- Herniated disc pressing on a nerve root.
- Bone spurs (osteophytes) from degenerative changes narrowing the neural foramen.
- Foraminal stenosis reducing the exit space for the nerve.
- Degenerative disc disease and facet joint hypertrophy.
- Less commonly, cysts, tumours, or infection affecting the nerve root.
How diagnosis is made
- Detailed neurological examination mapping the specific nerve root involved.
- MRI scan to identify the cause and level of nerve root compression.
- CT scan for detailed bony anatomy when foraminal stenosis is suspected.
- Electromyography (EMG) and nerve conduction studies for chronic or atypical cases.
- Selective nerve root blocks for diagnostic confirmation in complex cases.
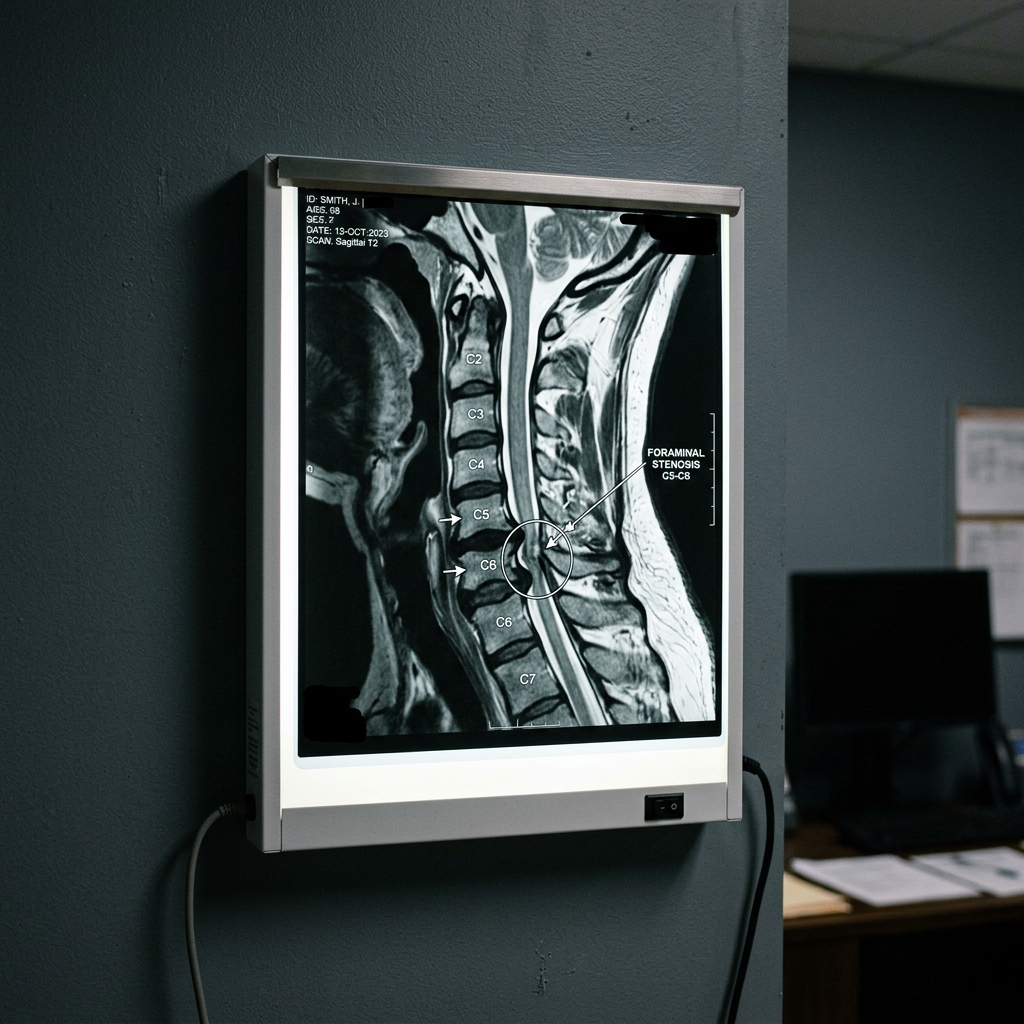 Typical diagnostic grey-scale imaging scan (MRI/CT).
Typical diagnostic grey-scale imaging scan (MRI/CT). Non-surgical treatment options
- Physiotherapy with cervical or lumbar traction, nerve mobilisation, and strengthening.
- Anti-inflammatory medications and neuropathic pain agents.
- Epidural or transforaminal steroid injections to reduce nerve root inflammation.
- Activity modification and ergonomic adjustments.
- Time and natural healing: many cases resolve within 6 to 12 weeks.
When surgery may be considered
Surgery is considered when significant symptoms persist despite 6 to 12 weeks of conservative management, or when there is progressive neurological deficit. Cervical radiculopathy may be treated with anterior cervical discectomy or disc replacement, while lumbar radiculopathy typically responds to microdiscectomy or decompression.
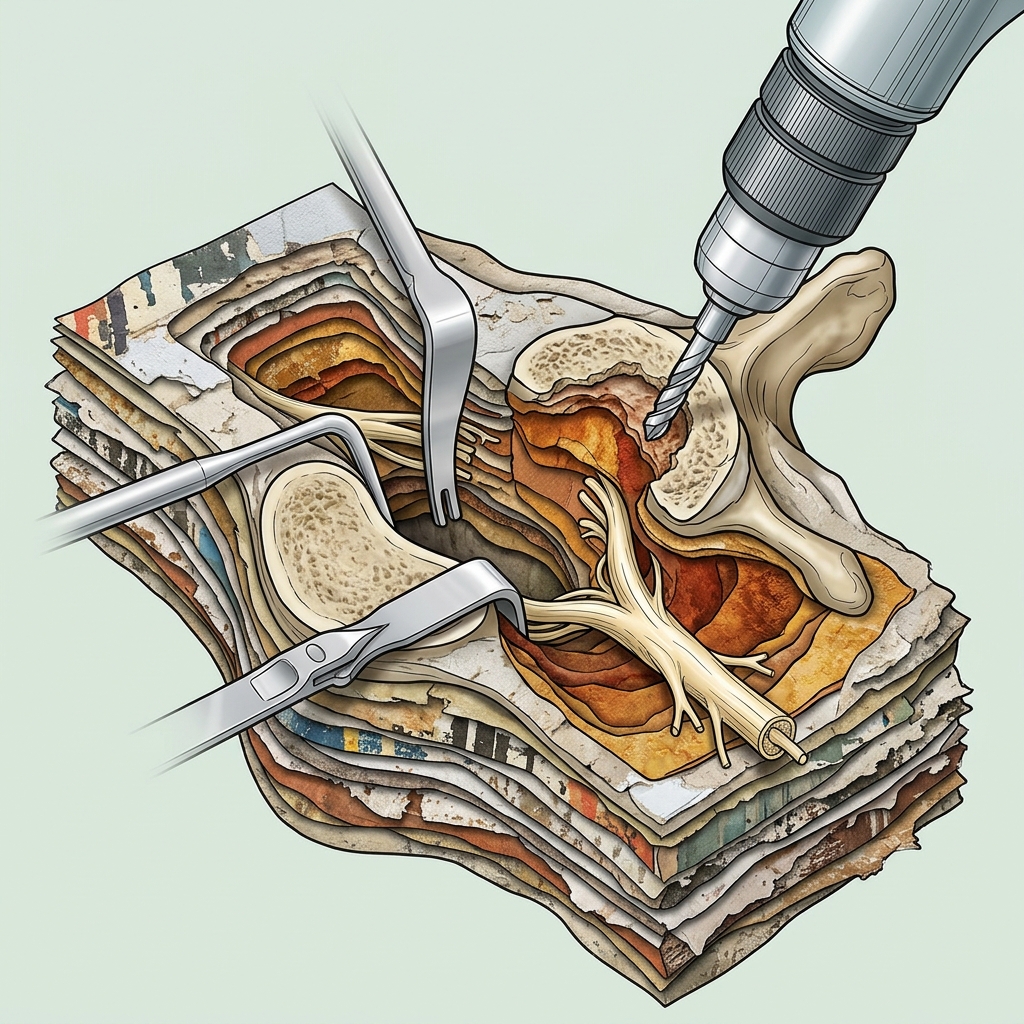 Advanced surgical technology and precision instrumentation.
Advanced surgical technology and precision instrumentation. Expected outcomes
Surgical decompression for radiculopathy has high success rates, typically exceeding 85 to 90% for relief of arm or leg pain. Most patients return to normal activities within 4 to 8 weeks of surgery.
 Rehabilitation pathways and safe movement restoration.
Rehabilitation pathways and safe movement restoration. Frequently asked questions
What is the difference between radiculopathy and sciatica?
Sciatica is a type of lumbar radiculopathy. Radiculopathy is the broader term for any nerve root compression in the spine, whether in the neck (cervical) or lower back (lumbar). Sciatica specifically refers to lumbar radiculopathy affecting the sciatic nerve.
Can radiculopathy be cured?
Many cases resolve completely with conservative treatment. When surgery is required, it is highly effective at relieving nerve root compression. The underlying degenerative changes remain, but the acute nerve compression can be durably addressed.